Ilioinguinal approach
(Modified)
Indication
Difficult acetabular fractures with anterior displacement in which access to the entire anterior column is required.
This approach allows access to the anterior column as far as the symphysis and includes the quadrilateral plate. Most both-column fractures can also be managed through this approach, but only if the posterior fragment is large and in one piece.
-
Anterior wall and anterior column fractures
-
Both-column
-
Anterior column posterior hemitransverse
-
Some transverse or t-type fractures.
Complications:
-
Interruption of the lymphatics with resultant limb oedema (1.6%)
-
Arterial thrombosis (0.5%)
-
Femoral nerve injury (1.1%)
-
Sciatic nerve injury (2.7%)
-
Inguinal hernia (0–1.1%)
Anatomy
The primary feature of the ilioinguinal approach is complete opening of the inguinal canal.
Three windows are developed to allow visualization of the acetabulum.
-
Lateral - between the iliac wing and the iliopsoas muscle
-
Middle - between the femoral nerve (iliopsoas muscle) and the external iliac vessels
-
Medial - between the lymphatics and the rectus abdominus at the level of the pubic tubercle
 (Click
on image for full size)
(Click
on image for full size)

Ilioinguinal deep anatomy
Considerations
In 1994, Cole and Bolhofner described the modified Stoppa intrapelvic approach for the treatment of acetabular fractures.
The primary feature of this approach is dissection along the pelvic brim with elevation of the iliopectineal and obturator fascias.
Direct visualization of the medial wall, dome, quadrilateral plate, and sacroiliac joint can be obtained.
Reported advantages of this
approach include an improved mechanical advantage in the reduction and fixation
of medially displaced fractures.
The modified ilioinguinal approach as described by Karunakar combines
features of both the ilioinguinal and modified Stoppa approaches.
Positioning
Supine with small sand bag or bunched up bean bag underneath the pelvis.
(must be able to get beyond the most lateral convexity of iliac crest, and across midline at pubic symphysis)
Supine (sloppy lateral)
Skin Incision
Begin 2 cm above and past the midline of the symphysis pubis.
Extend toward the anterior superior iliac spine in a curvilinear fashion.
Then carry it posteriorly along the crest beyond its most lateral convexity to permit adequate retraction of the iliopsoas and the abdominal muscles.
Superficial dissection
Develop the interval between the external oblique and the abductor muscles, exposing the iliac crest.
Deep dissection
Three windows are developed
-
Lateral - between the iliac wing and the iliopsoas muscle
-
Middle - between the femoral nerve (iliopsoas muscle) and the external iliac vessels
-
Medial - between the lymphatics and the rectus abdominus at the level of the pubic tubercle.
 (Click
on image for full size)
(Click
on image for full size)
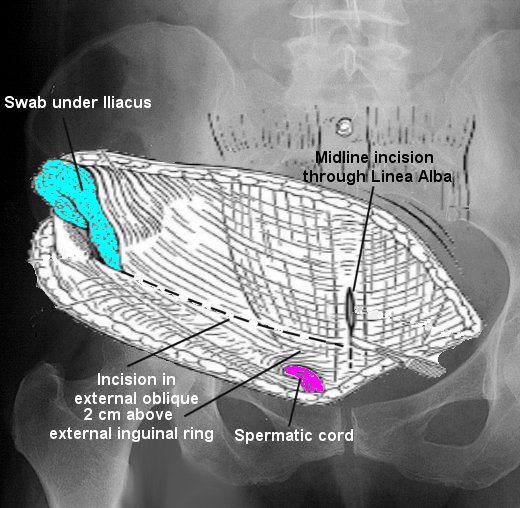
Figure 1.
Incision through external oblique aponeurosis, 2 cm above external inguinal ring
(Click
on image for full size)
Figure 2.
Developing three windows, deep anatomy
The lateral window
Dissect the iliacus muscle subperiosteally from the iliac crest, elevating it from the internal iliac fossa as far medially as the anterior aspect of the sacroiliac joint and distally to the iliopectineal eminence.
The nutrient foramen of the posterior and inferior part of the iliac fossa is located 1 to 2 cm from the sacroiliac joint and the pelvic brim.
This should be controlled by packing a lap sponge in the iliac fossa or by applying bone wax to the nutrient foramen.
The medial window
Begins with the same approach used for anterior symphyseal plating (Pfannenstiel).
Incise the linea albae down to the symphysis pubis.
Protect the bladder with a malleable retractor.
Subperiosteal dissection is performed along the pelvic brim (modified Stoppa).
The retropubic vascular system contains a large number of vascular anastomoses.
The majority of anastomoses include connections of the inferior epigastric and obturator vessels, ligated these as necessary with sutures or small vascular clips.
The corona mortis, the vascular
anastomosis between the external iliac and obturator vessels, may be encountered
in this dissection. If encountered ligate this vessel.
The external oblique fascia is exposed to the level of the rectus fascia.
It is incised from the anterior superior iliac spine (ASIS) to the midline 2 cm above the external inguinal ring.
Careful attention is paid to identifying the ilioinguinal nerve as it runs along the spermatic cord (male) or round ligament (female).
The superior limb of the external oblique fascia requires no elevation.
Elevate the inferior limb of the external oblique fascia gently along the entire course of the incision.
This provides exposure to the inguinal ligament (the inferior border of the external oblique aponeurosis with the internal oblique).
The inguinal ligament is incised sharply, preserving a 1 to 2 mm cuff of the ligament on the proximal side of the incision for later reattachment.
The incision is stopped 1 to 2 cm beyond the medial border of the iliopsoas to allow identification of the iliopectineal fascia.
Careful attention must be exercised
not to injure the structures lying directly beneath the inguinal ligament.
The lateral femoral cutaneous nerve passes through or immediately deep to the
inguinal ligament. The nerve usually passes immediately adjacent to the anterior
superior iliac spine but can be found at variable locations. The nerve should be
identified and mobilized prior to detachment of the inguinal ligament from the
ASIS.
The Middle window
The iliopectineal fascia must be released to provide exposure to the second window of the approach.
This fascia separates the femoral nerve from the external iliac artery and vein.
Retracting iliopsoas and femoral nerve laterally and the external iliac vessels medially provides exposure to the iliopectineal fascia so that it can be incised under direct vision to the iliopectineal eminence.
Blunt finger dissection can be used to further elevate the iliopectineal fascia off of the pelvic brim.
A penrose drain can be placed around the iliopsoas muscle, femoral nerve, and lateral femoral cutaneous nerve. Hip and knee flexion can be used to relax the iliopsoas tendon if further exposure is needed.
A second penrose is passed from the middle window to the
midline opening of the linea albae containing the external iliac vessels,
contents of the inguinal canal medial to the iliopsoas, and the affected side
rectus abdominus.
Exposure extension
To fully develop the medial (Stoppa) window, stand on the opposite side of the table to visualize the medial wall of the acetabulum. A headlight improves visualization inside the pelvis.
Dissection can be continued underneath the neurovascular structures (external iliac vessels) to the level of the sacroiliac joint.
A blunt Hohmann or malleable retractor can be placed against the ischial spine.
This provides excellent visualization of the medial wall of the acetabulum to the level of the ischial spine. The obturator nerve and vessel will be well visualized in the inferior portion of the wound and should be protected. If further exposure is necessary, a transverse incision through the aponeurotic insertion of the rectus abdominus may be made. This incision should be repaired at the completion of the procedure.
The original description of the ilioinguinal approach makes intraarticular visualization of the hip impossible. If visualization of the joint is required, a T extension of the incision just medial to the anterior-superior iliac spine can be made.
Most surgeons accept that the joint is reduced when the fracture lines inside the pelvis are reduced, and thus this extension is very rarely used.
Closure
Post operatively
References
Karunakar, Madhav A.; Le, Theodore T.; Bosse, Michael J.; The Modified Ilioinguinal Approach. Journal of Orthopaedic Trauma. 18(6):379-383, July 2004.
Letournel E. The treatment of acetabular fractures through the ilioinguinal approach. Clin Orthop. 1993;292:62–76.