Distal Humeral fractures
Fractures of the distal humerus account for 2% of all fractures and one-third of those at the elbow.
For diaphyseal fractures of the distal third of the humerus (see humeral shaft fractures)
Classification
Fractures of the distal humerus may be divided descriptively into:
-
Distal third of humerus (see humeral shaft)
-
Supracondylar (High and low supracondylar; flexion and extension)
-
Intercodylar (Intra articular)
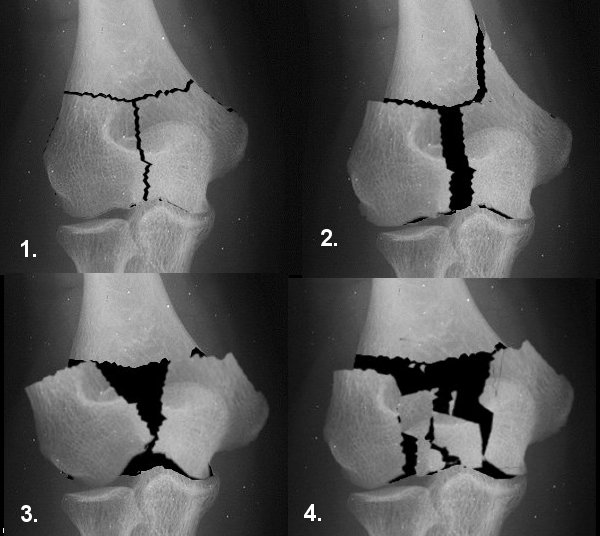
Riseborough and Radin
Described a series of intercondylar
T-fractures and divided them into four types reflecting severity as follows:
|
|
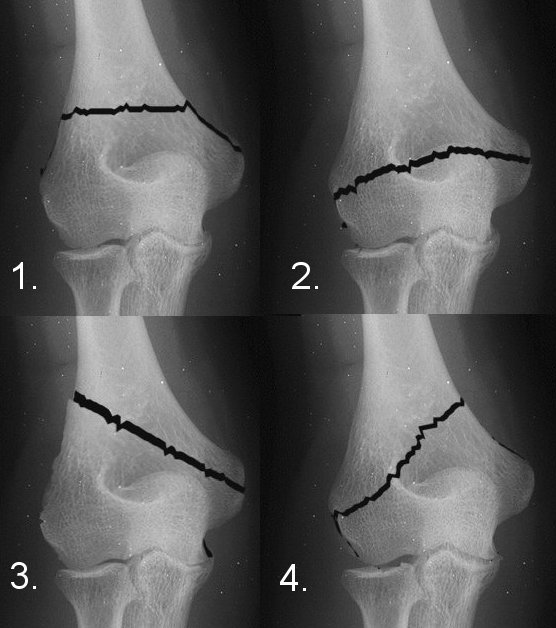
Type I. No displacement Type II. The trochlear and capitellar fragments are separated but not appreciably rotated. Type III. As for type II but the fragments are also significantly rotated. Type IV. Severe comminution of the articular surface and wide separation of the humeral condyles.
|
AO
 |
Humerus = 1 Distal segment = 3 Type B. Partial articular fractures; these maintain some continuity between the shaft and the articular surface. Type C. Complete articular fractures. These are then further subdivided subdivided into groups 1, 2 and 3 on the basis of the location of the line of the fracture and the amount of fragmentation. They in turn are further subdivided into subgroups •1, •2 and •3 by specific further qualifications. ( click on image for larger version) |
Jupiter and Mehne
Three basic categories:
-
Grade I. Intra-articular fractures
-
Grade II. Extra-articular, intracapsular fractures.
-
Grade III. Extracapsular fractures.
Intra articular fractures are subdivided into: single column; bicolumnar; capitellar; trochlear.
Grade I Intra-articular (Bi-column and single column)
|
Bi - column |
Single column |
||
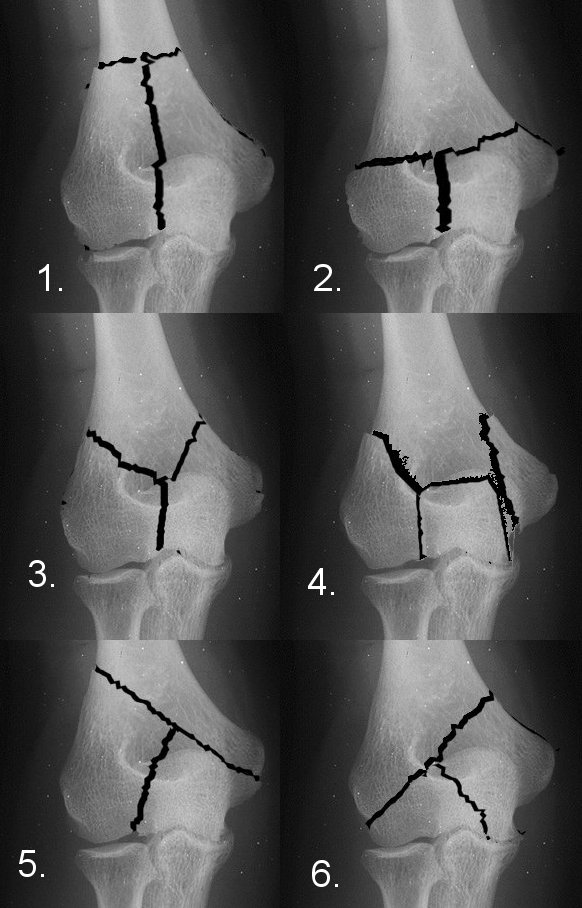 |
1. High T intercondylar 2. Low T intercondylar 3. Y intercondylar 4. H intercondylar 5. Lambda pattern (lateral) 6. Lambda pattern (medial) |
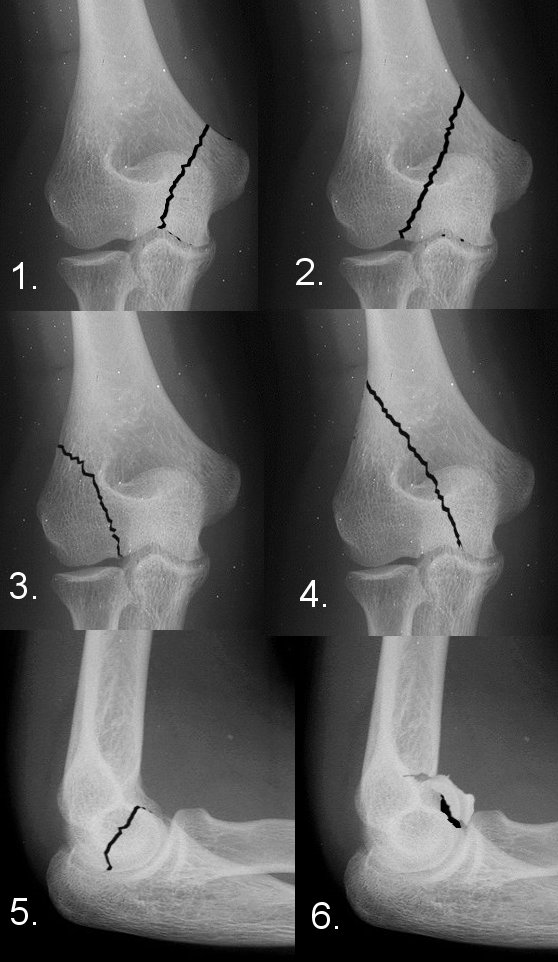 |
1. Low medial 2. High medial 3. Low lateral 4. High lateral 5. Capitellum 6. Trochlea |
Grade II Extra-articular - intracapsular
 |
1. High transcolumn 1a. extension, 1b. flexion 2. Low transcolumn 2a extension, 2b flexion 3. Abduction 4. Adduction |
Grade III Extra-capsular
 |
1. Medial epicondyle 2. Lateral epicondyle |
It can sometimes be difficult to classify on initial radiographs, radiographs in traction may help.
Treatment
Non operative
Operative
MUA and K-WIRE
ORIF
Arthroplasty
Non operative
Indicated for undisplaced fractures.
In elderly patients with osteopoenia and displaced fractures, careful decision making is required on non operative and operative intervention ORIF or Arthroplasty.
Operative treatmtent
MUA and K wiring is not a good solution for fractures around the elbow in adults.
Percutaneous screw fixation is possible for relatively stable single column fractures, Absorbable PDS pins and headless screws can be used for capitellar fractures.
ORIF requires considerable expertise and appropriate implants
Arthroplasty is indicated in multifragmentary fractures not reconstructible or in osteopoenic bone where the implant is not likely to hold till the fracture has healed.
External fixation may be used temporarily for severely contaminated open wounds.
Surgical approach
See surgical approaches to the elbow
Extraarticular fractures a triceps splitting approach is best, a paratricipital approach is possible.
Intra articular fractures require an anatomical reduction and rigid fixation.
Approaches include Olecranon osteotomy OR a triceps reflecting procedure, each have their own pro's and cons.
For Olecranon osteotomies an intraarticular chevron osteotomy is best to achieve stable fixation, intraarticular transverse osteotomies and extraarticular oblique osteotomies have a higher risk of non-union. (See Olecranon osteotomy).
Several methods of triceps reflection have been described
-
Campbell's Posterior Approach - Triceps aponeurosis and deep medial head, midline split. Gschwend modified this by elevating osteoperiosteal flaps.
-
Campbell triceps tongue - A tongue of triceps aponeurosis, left attached to the olecranon, is elevated with division of the deep head in the midline. Only indicated if patient has significant FFD requiring V-Y lengthening of triceps.
-
Alonso-Llames Approach - "bilaterotricipital approach", triceps is approached from medial and lateral aspects and elevated from each intermuscular septum. It allows for easy conversion to olecranon osteotomy if further exposure is required.
-
Bryan and Morrey Approach - Incision along medial aspect of the triceps, extending distally through the posterior bundle of the medial collateral ligament and joint capsule and then obliquely across the fascia over flexor carpi ulnaris, crossing the subcutaneous border of the ulna to the extensor carpi ulnaris, where it ends. This mandates anterior ulna nerve transposition. The triceps and fascia are elevated as one flap from medial to lateral. Variations include elevation of osteoperiosteal flap to avoid button holing thin fascia. Excise the tip of the olecranon to improve joint surface visualisation. Reflect the anterior medial collateral ligament by sharp dissection from the humerus, dislocate the elbow, providing exposure for a linked total elbow arthroplasty if needed.
-
Boyd Approach - Elevate the muscles on the lateral side of the ulna sub periosteally off the ulna. Retract anconeus and supinator to expose the joint capsule overlying the radial head and neck. This lateral capsule contains the lateral ligamentous complex and its division can lead to posterolateral rotatory instability.
-
Stanley posterior approach -Incise triceps tendon, with 75% of muscle lateral and 25% medial, continued distally to split the superficial fascia of the forearm for 6 or 7 cm. The medial triceps, with the superficial fascia of the forearm and the periosteum over the medial aspect of the olecranon, is then reflected medially as a single unit. Reflect subperiosteally, deep to the ulnar nerve and over the tip of the medial epicondyle, then reflect the lateral 75% of the triceps from the tip of the olecranon.
Principles of internal fixation
Two philosophies exist:
-
AO 90/ 90 plating
-
Restoring the arch concept
References
J. R. Williams, A. M. Wainwright, and A. J. Carr; Interobserver and intraobserver variation in classification systems for fractures of the distal humerus; JBJS - Br, Jul 2000; 82-B: 636.
Patterson, Stuart D. MBChB +; Bain, Gregory I. MBBS **; Mehta, Janak A. MS; Surgical Approaches to the Elbow. Clinical Orthopaedics & Related Research. (370):19-33, January 2000.
G.I. Bain, N. Ashwood, R. Baird, and R. Unni
Management of Mason Type-III Radial Head Fractures with a Titanium Prosthesis,
Ligament Repair, and Early Mobilization
J Bone Joint Surg Am. 2005;87(Supp 1):136-147
S. A. Shahane and D. Stanley; A posterior approach to the elbow joint; J Bone Joint Surg Br, Nov 1999; 81-B: 1020
Anglen J.; Distal humerus fractures.; J Am Acad Orthop Surg. 2005 Sep;13(5):291-7. Review.