Acetabular fractures
Joint congruity is essential.
If closed reduction fails, then open reduction is essential.
Open reduction will improve results
only if anatomic reduction is achieved and complications are avoided.
Anatomic reduction does not ensure a good result viz. cartilage damage.
Mechanism of Injury
Consider position of femoral head, ie. internal rotation forces it against the posterior column etc.
Seperate the low energy injury in the elderly from the high energy injury in younger patients.
Radiology

Inverted Y, one limb the anterior column and one the posterior column.
The anterior column extends from the iliac crest to the symphysis pubis and includes the anterior wall of the acetabulum.
The posterior column begins at the top of the sciatic notch; descends through the acetabulum, obturator foramen, and inferior pubic ramus; and includes the posterior wall and the ischial tuberosity.
The dome or roof is the superior weight-bearing area, which includes a portion of both the anterior and posterior columns.
Radiographs
The anteroposterior view gives a preliminary understanding of the fracture pattern. The oblique views confirm initial impressions and provide detail.
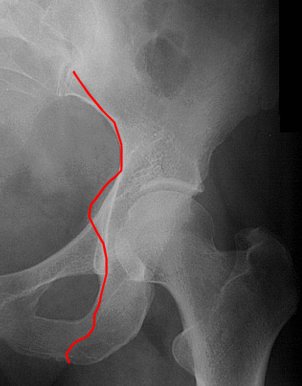
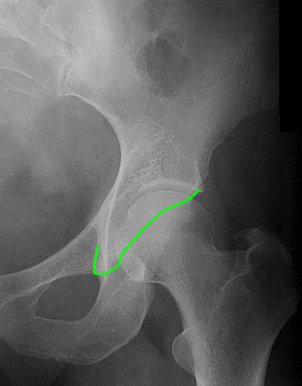
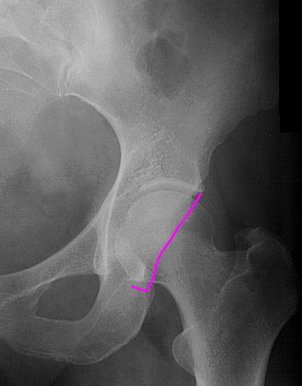
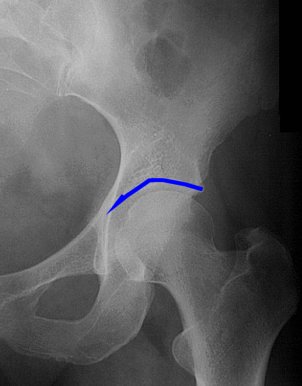
- AP pelvis (look at below)
|
Iliopectineal line (anterior column) |
Ilioischial line (posterior column) |
Anterior lip and teardrop |
Posterior lip | Dome |
 |
 |
 |
 |
 |
-
Judet views
45° obturator oblique - Anterior column, posterior wall
45° iliac oblique - Posterior column, anterior wall
Analysis of the fracture begins with the anterior-posterior hip view:
-
A break in the iliopectineal line indicates a break in the anterior column.
-
A break in the ilioischial line indicates a break in the posterior column.
-
Discontinuity in the posterior lip suggests a posterior wall fracture
-
Discontinuity of the anterior lip suggests an anterior wall fracture.
-
A break in the obturator ring suggests a fracture separating the anterior and posterior columns.
Computed tomography
Shows steps, gaps and intra articular loose fragments better than radiographs.
Classification
Most current classifications are anatomic and do not consider the other essential factors in decision making:
- Degree of displacement
- Comminution
- Exact location of fracture lines
-
State of the bone
Thus, the fracture classification
should never be used in isolation to develop a treatment plan or surgical
tactic.
The anatomic classifications can be simplified by recognizing that the acetabulum has only so many parts that can break:
- Two columns, an anterior and a posterior
- Two walls (lips), anterior and posterior
The acetabulum is made up of two columns (anterior and posterior) and two walls (anterior and posterior).
All of the fracture types other than the so-called both-column type are permutations and combinations of that anatomy.
Thus:
-
A: the anterior column may be fractured, the posterior column fractured, or both columns fractured together (transverse fracture). The T fracture is a transverse component with both columns separated from each other.
-
B: The anterior wall may be fractured, a lesion often associated with anterior dislocation, or the posterior wall may be fractured, almost inevitably with posterior dislocation of the hip. These fractures may occur in isolation or in combination, with anterior column and posterior column fractures as well as transverse and T fractures.
-
C: The both-column fracture, by definition, divides the ilium proximal to the hip joint; therefore, no portion of the articular surface of the hip remains attached to the axial skeleton. In reality, this both-column fracture is a type of T fracture occurring proximal to the joint.
Letournel and Judet classification (1993)
Divided all the fractures into simple (elementary) and associated types.
Simple (elementary)
-
Anterior wall
Anterior column
Posterior wall
Posterior column
Transverse
Associated
-
T-shaped
Anterior wall/column plus posterior hemitransverse
Transverse plus posterior wall
Posterior column plus posterior wall
Both-column
Beaulé et al showed, Letournel's acetabular classification with use of plain radiographs with or without supplemental computed tomography scans has substantial reliability (Kappa > 0.7) when used by surgeons who have been taught how to interpret the images or by those who treat acetabular fractures on a regular basis.
The value of computed tomography scans in the evaluation of acetabular fractures has been well established for the identification of loose bodies and articular impaction; however, they do not appear to be essential for the classification of acetabular fractures.
Universal comprehensive classification
This classification, developed with the help of Letournel, Matta, Helfet, and others, has received international recognition from International Society of Orthopaedic Surgery and Traumatology (SICOT), the Orthopaedic Trauma Association (OTA), and the AO group.
It does answer some of the questions of prognosis with the modifiers, but acetabular fractures are so complex that there are still some deficiencies; for example, many of the type B fractures are high-energy, shearing fractures with a worse prognosis than the both-column type C fractures.
However, this classification is comprehensive, is universal, and should be used for case comparison by different centres.
Its structure is analogous to that of the AO comprehensive fracture classification, which groups all fractures into A, B, and C types with severity increasing toward the C type.
In the comprehensive acetabular
fracture classification, these types are anatomic, based on the Letournel-Judet
classification, and modifiers are used to denote prognostic indicators
identified by Greek letters.
PITFALLS IN DIAGNOSIS
Prolonged dislocation of the femoral head may increase the rate of aseptic
necrosis.
Therefore, it is essential to recognize and address hip dislocations promptly.
Occasionally the radiographs can be deceptive. A femoral head that is dislocated posteriorly will sometimes look as if it is in the acetabulum. To recognize this situation, remember that the located hip will appear approximately congruent beneath the dome even in the presence of a posterior wall fracture. When the posterior wall fracture is large, it may be impossible to keep the head located beneath the dome. In these cases, traction should be used to maintain reduction of the femoral head.
Large femoral head impaction fractures frequently lead to a poor result.
Thus, in a few cases it may be advisable to choose a less extensive approach to
avoid complications that may impair late reconstructive procedures.
Marginal impaction is commonly associated with posterior wall fractures. Even
though the presence of marginal impaction increases the risk for a poor outcome,
it should not be used as an excuse for a poor reduction. It is essential to
recognize the marginal impaction preoperatively so that it can be addressed at
the time of surgery.
Surgical anatomy
Posterior Wall Fractures
Posterior wall fragments vary in size and the degree of comminution.
In most cases, the degree of comminution can be appreciated preoperatively on
the CT scan. However, it is not unusual to find additional fracture lines at the
time of surgery. The surgeon should be prepared to manage a fracture with
multiple fracture lines even when the fracture appears straightforward on the CT
scan. In addition, because of these potentially unrecognized fracture lines, a
posterior wall fracture should never be fixed with lag screws alone.
Free osteochondral fragments frequently accompany posterior wall fractures. When
these pieces are small and out of the weight-bearing area, they can be
discarded. However, when they are large (as is usually the case) they should be
returned to their anatomic location. Doing so may involve significant “fiddle,”
but resist the notion that somehow the pieces will no longer
fit back together. In a closed posterior wall fracture, no fragments leave the
body, so it is always possible to return the wall to its original anatomy. In
the same vein, marginally impacted fragments should be identified, elevated, and
grafted.
Remember the posterior wall fragment receives its blood
supply from the capsule. To visualize and debride the joint, the fragment should
be flipped up on its capsular attachment. Avoid detaching the fragment from its
blood supply.
Posterior Column Fractures
Posterior column fractures can occur anywhere along the posterior column from the ischial spine to the sciatic notch. Typically, the column fragment rotates, making reduction difficult. At the time of surgery, it is necessary to de-rotate the fragment and to check the reduction on the inside and the outside of the pelvis.
Anterior Column Fractures
These fractures occur at various levels along the anterior column. Although the pubic ramus is part of the anterior column, isolated ramus fractures generally indicate the presence of a pelvic fracture rather than an acetabular fracture.
Transverse Fractures
Transverse fractures run across the acetabulum.
Fracture in the region of the fovea = infratectal.
Fracture just above the fovea = juxtatectal
Fracture crossing higher = transtectal.
Typically, there is greater displacement posteriorly than anteriorly, but this is not always the case. Make note of the area of greatest displacement. Fractures with the greatest displacement posteriorly are difficult to reduce from anterior approaches, and the reverse is also true.
T-Type Fractures
T-type fractures are simply transverse fractures with a fracture line separating the anterior column from the posterior column. The inferior limb can exit at various locations. T-type fractures are similar to transverse fractures in that displacement can be greater anteriorly or posteriorly.
Anterior with Posterior Hemitransverse Fractures
These fractures are frequently confused with T-type fractures; however, there are important differences. In essence, the pattern is an anterior column fracture with an additional fracture line that runs transversely across the posterior column. Most of the displacement is usually anterior, and the posterior capsule is not significantly disrupted. Thus, reducing the anterior column generally reduces the posterior column. In T-type fractures, the posterior capsule is frequently disrupted so the posterior column does not necessarily reduce with the reduction of the anterior column.
Both-Column Fractures
The both-column fracture should not be confused with other fractures in which both columns are fractured.
Both columns are disrupted with transverse, T-type, and anterior with posterior hemitransverse fractures, but none of these is considered to be a both-column fracture.
In the both-column fracture, the entire acetabulum is separated from the axial skeleton. It is sometimes called a floating acetabulum. Because the entire acetabulum is separated from the ilium, the actual joint can appear very congruent. This radiographic finding is known as secondary congruence.
Biomechanics
Although most surgeons agree that it is critical to reduce displaced fractures that cross the weight-bearing area, the portion of the acetabulum necessary for normal weight bearing is not truly known. One way to define the weight-bearing area is as the portion of the acetabulum that is necessary to maintain hip stability. Using this definition, the weight-bearing area is primarily posterior and superior. During normal gait, peak forces cross the acetabulum in this region, so it makes sense that this area would be critical for weight bearing.
Posterior wall fractures affect stability depending on their size.
- Less than 20% of the posterior wall does not affect stability
- More than 40% always render the hip unstable
- Clinical evaluation helps to determine stability between these extremes
Excessive pain when the hip is flexed with the patient awake suggests instability. If a question remains, the hip can be evaluated under anaesthesia. The hip should be stable through flexion to 100° in 10° of adduction.
TREATMENT OPTIONS
There are two basic treatment options:
- Operative
- Nonoperative
In a young, healthy patient, open reduction and internal fixation (ORIF) may be appropriate. In an older patient with severe femoral head damage, ORIF with a concomitant total hip arthroplasty may be best. Furthermore, either traction or full weight bearing may be selected for nonoperative management. The ultimate decision is based not only on a detailed analysis of the fracture but also on the patient's overall health, associated injuries, and the surgical risks. In addition, surgeons should be realistic about their abilities. Generally, these are complex fractures, and achieving optimum results requires experience. Nevertheless, it is useful to consider indications specific to the fracture for operative and nonoperative management.
The desirability of surgery is based on its ability to restore hip joint stability and congruity of the weight-bearing acetabulum. The most definitive indication for surgery is instability of the hip joint. If the hip is clearly subluxated on any of the radiographic views, surgery is indicated. It is important to make this determination with the patient out of traction. Traction may bring the femoral head under the intact dome without reducing the fracture. The fracture will heal in a displaced position, and as soon as the traction is released, the hip will subluxate. Similarly, surgery is indicated if the hip is grossly dislocated on clinical exam.
The decision is more difficult when the hip appears congruent even with the
patient out of traction. Clearly some fractures are so low that they will not
affect weight bearing. Other fractures are high enough to cause frank
dislocation. In between these two extremes, the hip may be located with the
patient at rest but dislocate or subluxate during normal weight bearing. The
classic example is a large posterior wall fracture. With the patient supine, the
hip will remain located beneath the dome. However, as soon as the hip is flexed,
the femoral head falls out the back. For these fractures, the decision of
whether or not to operate is based on the size of the posterior wall fragment
and on the location of the fracture relative to the weight-bearing dome. A
displaced fracture crossing the weight-bearing dome is an indication for
surgery.
The radiographic roof-arc angle is frequently used to define the weight-bearing
dome.
 |
Draw a vertical line through the rotational centre of the acetabulum Draw a second line through the rotational centre of the acetabulum to the point where the fracture crosses the radiographic dome. The roof-arc angle is the angle created where these lines cross. |
Matta suggests that a
fracture will cross the weight-bearing dome if the roof-arc angle is less than
45°on any of the three standard radiographic views. Recent biomechanical
evidence suggests that a fracture crosses the weight-bearing area if the
anterior roof-arc is less than 25°, the medial roof-arc is less than 45°, or the
posterior roof-arc is less than 70°.
The roof-arc angle can be difficult to measure accurately, and, if the patient
is not perfectly positioned when radiographs are taken, roof-arc angles can be
misleading. Alternatively, the CT scan can be used to evaluate the
weight-bearing area. Olson and Matta suggest that the CT cuts from the top
of the dome and distally for 1 cm define the weight-bearing dome. Therefore, if
the fracture is visible on any of these cuts, it must cross the weight-bearing
area. Another option is to define the weight-bearing area as shown in. Any fracture line crossing this area would be in the weight-bearing
portion of the acetabulum.
Closed treatment is reasonable, even for fractures crossing the weight-bearing
dome, when the displacement is less than 2 mm. However, the patient should be
treated in traction to prevent further displacement or followed closely to catch
any displacement that might occur. Surgery may be considered to prevent
displacement if it can be done with acceptable risk.
Age alone should not be a contraindication for ORIF. Results for total hip
arthroplasty after unreduced acetabular fractures are not as good as those for
primary total hips or for those following ORIF of acetabular fractures. In addition, one can expect the results of ORIF in older patients to
mirror those for younger patients for similar surgery. Nevertheless, the
surgeon should take care not to jeopardize future reconstructive procedures with
overly aggressive attempts at reduction when other factors that increase the
likelihood of a poor result are present.
SURGICAL CONSIDERATIONS
If possible, surgery should be completed within the first 7 days. The earlier the surgery, the easier the reduction. Results do not begin to deteriorate until the operation has been delayed 3 weeks.
However, a delay may obligate the surgeon to a more extensile exposure, thereby increasing the complication risk. Emergency surgery is rarely indicated. These procedures are difficult and must be done under optimal conditions, but occasionally they are done emergently for irreducible dislocations, increasing neurologic deficits, or a vascular injury. Prophylactic antibiotics are given. Adequate amounts of blood must be on hand and the use of a cell-saver device is desirable. Neurologic monitoring may decrease the risk of iatrogenic nerve injury, especially for late cases (>3 weeks from injury).
SURGICAL APPROACHES
The type of fracture mainly determines the choice of incision, but other factors also influence the choice.
The general trend is towards more limited exposures to avoid the complications of the more extensile ones. When possible, anterior approaches are preferred to posterior approaches because of the lower incidence of heterotopic ossification.
The full triradiate, the extended iliofemoral, and combined approaches are now primarily used for late cases. However, the surgeon must remember that anatomic reduction is the goal.
A limited exposure does no good if the fracture is not reduced and fixed properly.
Iliofemoral
For fractures of the anterior column in which the main displacement is cephalad to the hip joint, the iliofemoral approach is sufficient. This approach does not allow access distal to the iliopectineal eminence, but if the fracture occurs above it, this incision may be used. Adduction and internal rotation of the hip joint may increase the exposure. Lag screw compression-fixation of an anterior column fracture is possible through this approach, but it is not possible to place a plate along the full pelvic brim. Plates may be used on the crest of the ilium for fixation. This approach, therefore, is used for anterior column and anterior wall fractures with no extension distal to the iliopectineal eminence.
Ilioinguinal
For difficult fractures with anterior displacement in which access to the entire anterior column is required, the ilioinguinal approach is ideal. This approach allows access to the anterior column as far as the symphysis and includes the quadrilateral plate. Most both-column fractures can also be managed through this approach, but only if the posterior fragment is large and in one piece.
The original description of the ilioinguinal approach makes intraarticular visualization of the hip impossible. If visualization of the joint is required, a T extension of the incision just medial to the anterior-superior iliac spine can be made. Most surgeons accept that the joint is reduced when the fracture lines inside the pelvis are reduced, and thus this extension is very rarely used.
Kocher-Langenbach
For isolated posterior wall injuries as well as posterior column injuries, a Kocher-Langenbach approach is indicated. This allows access to the posterior column and posterior wall only, but exposure is limited proximally by the superior gluteal vessels and the greater trochanter with the attached hip abductors.
In all posterior approaches, the sciatic nerve is in jeopardy; therefore, caution is advised. To protect it, the knee must be flexed at all times. Careful retraction using the muscle bellies of the short external rotators for protection is essential.
Injury to the superior gluteal artery and nerve must be avoided. They can be visualized exiting from the greater sciatic notch and in that location can be injured during stripping of periosteum.
If injured, the artery may bleed massively. In almost all cases, the bleeding will stop if the artery is packed for 20 minutes. In the rare case that bleeding does not stop, embolization or direct surgical ligation may be necessary. The superior gluteal nerve is closely associated with the artery. Indiscriminate clamping of the artery in the greater sciatic notch may injure the nerve; therefore, doing so should be avoided unless the artery is clearly visualized and isolated.
In cases in which the surgeon may choose either the anterior or posterior approach, preference should be given to the anterior approach because of a lower incidence of heterotopic ossification and risk to the sciatic nerve.
The trochanter can be removed to increase access to the superior acetabulum. This is occasionally necessary when a posterior wall fracture extends very high into the dome, but usually adequate visualization can be achieved by abducting the lower extremity. Removing the trochanter does provide some visualization of the anterior column but does not provide adequate access to reduce large displacements or to safely insert an anterior column screw.
Triradiate
For fractures in which both columns have been injured, the triradiate approach offers excellent exposure of the entire outer table of the pelvis from the anterior-superior spine to the top of the sciatic notch. It does not provide access to the bone above the sciatic notch.
Extended Iliofemoral
The extended iliofemoral approach gives excellent visualization of the outer table of the ilium, the superior dome, and the posterior column. The anterior column can be visualized to the iliopectineal eminence. The exposure is similar to that provided by the triradiate approach with the additional benefit of access to the bone above the sciatic notch. The approach can be extended to provide exposure to the iliac fossa; however, this is very rarely necessary and should be avoided. Extending the approach to the inside of the pelvis greatly increases the risk of devascularizing segments of the acetabulum.
Combined Anterior and Posterior Approaches
Simultaneous combined anterior and posterior approaches are possible. Winquist reported on 103 acetabular fractures managed by simultaneous anterior and posterior approaches when necessary. They had excellent ability to achieve anatomic reduction. If combined approaches are used, the patient is placed in the lateral position, with no fixed supports. This allows the surgeon to roll the patient prone or supine as necessary.
Although direct visualization of both columns through a single extensile approach is desirable, the complication rate in many reports is high, leading to a resurgence of interest in simultaneous combined approaches. However, the combined approaches may not greatly differ in complications; therefore, at this time, the decision must lie with the surgeon's preference and experience.
SPECIFIC FRACTURE TYPES—GUIDELINES FOR CHOICE OF APPROACH
Type A—Partial Articular Single Wall or Column
An isolated posterior wall fracture (A1) is best approached through a Kocher-Langenbach approach with the patient in the prone or lateral position. Positioning the patient prone allows gravity to keep the head reduced while the fracture is fixed, but most surgeons are more comfortable with the anatomy when the patient is positioned in the lateral decubitus.
For the A2 posterior column or posterior column/posterior wall fracture, the same approach as used for posterior wall fracture may be employed. For these fractures, it is best to position the patient prone. When the patient is in the lateral decubitus position, the weight of the leg causes the posterior column to rotate, making reduction more difficult.
For anterior wall and anterior column fractures (A3), the anterior iliofemoral approach may be sufficient if the column fracture is high, but for more distal anterior wall or low anterior column fractures, the anterior ilioinguinal approach is usually required.
Type B—Partial Articular—Transverse or T Types
For transverse and transverse/posterior wall fractures, the optimal approach depends on fragment rotation, displacement, and whether or not a posterior wall fragment is present. A significant posterior wall fragment mandates direct posterior visualization. If the posterior wall is intact, the approach will depend on the rotation of the fracture: if the gap is anterior, an anterior approach should be used; if it is posterior, then a posterior approach is used. When there is significant displacement both anteriorly and posteriorly, the surgeon should consider a more extensile exposure. These severely displaced fractures can be managed through more limited exposures, but doing so generally requires the expertise of an experienced acetabular surgeon.
Type B2 fractures (T types) are the most difficult fractures to treat surgically. They require a very experienced surgeon, and even then achieving anatomic reduction is difficult. The choice of incision requires much thought and is often dependent on the philosophy of the surgeon. In acute fractures, the trend is to simpler or combined approaches rather than extensile approaches (extended iliofemoral, triradiate), but in late cases the extensile approach may be necessary.
The type B3 fracture—anterior column with posterior hemitransverse fracture—can usually be fixed through an anterior ilioinguinal approach. Frequently, the posterior column is minimally displaced. Even when the posterior column is displaced, it generally reduces with reduction of the anterior column.
Type C—Complete Articular—The Both-Column Fracture (Floating Acetabulum)
If the posterior column fracture is a large single fragment, as is often the case, the preferred approach is the anterior ilioinguinal. The first step in the procedure is fixation of the large anterior fragment to the ilium, thereby restoring stability to the hemipelvis. Once the anterior column is reduced, the posterior column requires only slight further reduction. The posterior column is then stabilized by lag screws placed along the pelvic brim. If reduction or fixation of the posterior column proves impossible, be prepared to flip the patient over and approach the posterior column directly. If there is a significant fracture of the posterior wall, choose an extensile approach or combined anterior and posterior approaches. For delayed late reconstruction, the extensile approaches are preferred.
REDUCTION
Reduction is the most difficult aspect of acetabular surgery even with good exposure. To achieve an excellent reduction, the surgeon must have adequate personnel and material resources. These include at least two, and occasionally three, assistants, and special instruments manufactured specifically for this purpose. Reduction may be facilitated by the surgeon's use of many tactics, including traction, special clamps, and cerclage wires.
Traction is essential to reduce these fractures. Traction may be obtained
with a traction table, direct pull on the femoral neck, or external distractors.
The use of a traction table is controversial. It is strongly recommended by
Letournel for all cases and may reduce the need for some assistants. The
operating room table must be versatile enough to allow traction in all
positions—anterior, lateral, and posterior. An unscrubbed surgeon or operating
room technician with knowledge of the function of the table is essential
throughout the procedure.
Most patients can be handled without a traction table. The involved leg is
draped free to allow full movement and traction is provided when necessary by an
extra assistant. A table that allows full image intensification of the
acetabulum in multiple planes should be used. The use of an image intensifier
C-arm during the case greatly reduces the risk of placing a screw in the joint.
Direct traction through a corkscrew placed intraoperatively into the femoral
neck will allow good visualization of the articular surfaces. A
wide capsulotomy, detaching the capsule from the rim of the acetabulum, is
necessary when full joint exposure is required. A sharp hook placed around the
greater trochanter or, if the greater trochanter is osteotomized, into the
piriformis fossa affords excellent traction.
Rotational displacements of the posterior column and transverse and T-type
fractures can be difficult to correct when these fractures are approached
posteriorly. A 5- or 6-mm Schanz threaded pin inserted on a T-handle into the
ischial tuberosity provides a handle to address rotation.
The surgeon must be well versed in the use of the specialized clamps that have
been designed specifically for acetabular surgery. The pointed reduction clamps
are essential. When necessary, the clamp tips can be seated in drill holes or on
washers to provide more secure fixation. Farabeuf clamps may be used on screws inserted on either side of the
fracture. The other specialized clamps have specific uses with
different approaches. The offset clamps are used through the greater sciatic
notch to reduce the posterior column, whereas the large, two-pronged clamp is
used to hold the anterior column fragment in a both-column fracture through an
anterior approach.
A cerclage wire inserted through the greater or lesser sciatic notch can be a
useful reduction tool also. In some instances, the wire may be retained to also
help with fixation.
Marginally impacted articular fragments must be reduced. These fragments are
relatively common in joint dislocations. At surgery, the fragments can be
rotated 90 degrees so that the surgeon is looking directly at the articular
surface. The fragments must be de-rotated and grafting material placed behind
them as a buttress.
FIXATION TECHNIQUES
Implants
Stable internal fixation is best achieved by interfragmentary lag screws. In the
pelvis, 3.5-mm cortical screws are most often used. The shaft diameter of these
screws is larger than that of 4.0-mm cancellous screws, and since the cancellous
bone is dense, the fixation of cortical screws is good. It is not necessary to
tap for these screws except in the dense cortical bone of the sciatic buttress.
Screw lengths up to 120 mm must be available.
Plates are used to neutralize the fracture once reduction has been obtained and
the fragments fixed with lag screws. The 3.5-mm reconstruction plate is the
implant of choice for acetabular reconstruction. These plates can
be obtained either straight or curved and are easy to contour. They are fixed
with the 3.5-mm cortical screws.
Sites of Application
The plates may be applied to the anterior column from the inner table of the ilium to the symphysis pubis. Plates may also be applied to the posterior column. On the posterior column, the distal end should be secured to the ischial tuberosity. Great care should be taken to ensure that screws in the central portion of the plate do not penetrate the articular cartilage of the acetabulum. In most instances, no screws should be put into that danger area, and all screws in that area should be directed away from the joint. Screws within the joint are a not uncommon cause of chondrolysis. A plate should always be used to buttress posterior wall fractures. Lag screws alone do not provide durable fixation. For the buttressing of a fragmented posterior wall fragment or a large significant quadrilateral plate fragment, spring plates can be useful. A spring plate is made by cutting a three-hole, one-third tubular plate through the end hole. This leaves small tines that can be cut into points and bent 90 degrees to the plate. The plate is then concaved slightly and placed over the fragment. The pointed tines of the spring plate are placed in the bone at the rim of the acetabulum. The plate is secured with a screw through the next hole.
In many situations, screws alone provide the only fixation. For example, in a both-column fracture fixed through an anterior ilioinguinal approach, the posterior column is fixed with lag screws placed from the pelvic brim into the posterior column. Conversely, the anterior column in a transverse or T-type fracture is frequently stabilized by a long lag screw placed down the anterior column. In both of these circumstances, the potential for penetration of the hip joint is great, so caution is advised. Intraoperative fluoroscopy should be used to confirm that screws do not penetrate the articular surface. If any view shows the screw clearly out of the joint, then the surgeon can be sure that the screw is safe.
POSTOPERATIVE CARE
Suction drains are left in the wound for 48 hours. Indomethacin is used in the postoperative period to prevent heterotopic ossification. Low molecular weight heparin or warfarin (Coumadin) is used to prevent thromboembolic disease.
Postoperative mobilization depends on the quality of the bone, the adequacy of reduction, and the degree of stability for the internally fixed fracture. In most cases, the patient no longer requires traction after surgery. Patients remain non–weight bearing for 6 to 8 weeks and continue partial weight bearing for an additional 4 weeks. However, if the surgeon feels the fixation is tenuous or if large impacted dome fragments have been repaired, it is prudent to leave the patient in traction for 6 to 8 weeks.
During the period when the patient is non–weight bearing, active and active assisted range of motion is encouraged. Initially this is supervised by a physical therapist. However, once the patient has demonstrated the ability to work on range of motion independently, therapy visits are discontinued until the patient is full weight bearing. Once the patient is full weight bearing, aggressive therapy for gait training and muscle strengthening is required and the therapy visits are reinstated.
COMPLICATIONS
Complications associated with acetabular fractures are common. General complications include thromboembolic disease and infection. Wound problems are more common in the extensile approaches; therefore, careful patient selection is essential. The more specific complications are as follows.
Nerve Injury
Sciatic Nerve
Thirty percent of acetabular fractures have associated sciatic nerve injury. This high incidence mandates a careful neurologic evaluation in every case. The peroneal division is injured most commonly, but both divisions can be involved. Partial injuries increase the risk that the nerve will be injured during surgery.
The risk for iatrogenic injury is substantial, especially for posterior approaches. Intraoperative monitoring of nerve function may help to reduce the incidence, but some argue that experienced surgeons can achieve equally low rates without it. In any case, it is clear that experience is important. The surgeon must be extremely vigilant throughout the case, monitoring retraction of the sciatic nerve, which is necessary for adequate exposure. Most importantly, the surgeon must ensure that the hip remains extended and the knee flexed whenever the nerve is retracted. Letournel and Judet reported an 18.4% rate of sciatic nerve injury in their original series of posterior approaches for acetabular fractures. Simply by keeping the knee flexed throughout the case, the incidence was reduced to 10%, and for their last 211 Kocher-Langenbach exposures, they reported a 3.3% incidence.
Femoral Nerve
Femoral nerve injury is rare either from the injury or surgery. Great care must be taken during the anterior ilioinguinal approach since the nerve is directly exposed.
Superior Gluteal Nerve
The superior gluteal nerve is vulnerable in the greater sciatic notch, where it may be injured during trauma or during surgery, resulting in paralysis of the hip abductors, creating a major disability.
Other Nerves
Other nerves can be injured. The pudendal nerve can be compressed on the traction table, but it usually recovers. Also, the lateral femoral cutaneous nerve is commonly stretched or cut during anterior approaches. The patient usually tolerates the sensory loss on the lateral aspect of the thigh but should be warned preoperatively about the likelihood of it occurring.
Heterotopic Ossification
Heterotopic ossification remains a problem, but as collective experience has increased, the incidence of significant heterotopic bone formation has decreased. Currently, most surgeons try to prevent heterotopic bone formation with indomethacin in a dose of 25 mg t.i.d. However, equally low rates may be possible without prophylaxis. Moed and Maxey found that indomethacin reduced the incidence of heterotopic ossification. Matta reported a 9% incidence of significant heterotopic ossification without prophylaxis. Johnson et al. however, reported a 62% incidence of Brooker grade III or IV heterotopic ossification for extended iliofemoral approaches when no prophylaxis was used. Although it may be possible for very experienced surgeons to avoid the use of prophylaxis, it seems prudent for most surgeons to use it in most cases. Radiation alone or in combination with indomethacin is very effective at preventing ectopic ossification. However, because the long-term risks of radiation therapy are unknown, most surgeons choose to use radiation only in select high-risk cases.
Infection
The incidence of infection is related to the surgeon's experience. Letournel reported an overall incidence of infection over 30 years of acetabular fracture of 4.2%. However, he noted that infections occurred primarily during two periods of his experience. In the early days, before he completely understood the pathoanatomy, he had numerous bad infections. The second peak came with his early experience with the ilioinguinal approach. In his first 22 ilioinguinal approaches, he had a 32% incidence of infection. For the next 146 cases subsequent ilioinguinal approaches the rate was 1.4%. The inexperienced surgeon should take heed.
The successful treatment of infection requires early recognition and aggressive management. When serosanguineous drainage continues for more than 4 days, the patient should return to the operating room for irrigation and debridement of the wound. This complication is not unusual, so the patient should be warned in advance. Matta reported a 5% incidence of infection but was able to manage these cases successfully with early aggressive debridement. However, Matta's experience is exceptional. We have had cases in which the treatment of infection was unsuccessful until all implants and necrotic bone had been removed.
Chondrolysis
Chondrolysis after acetabular trauma can occur with or without surgical intervention. Without surgical intervention, it is usually a manifestation of early osteoarthritis. After open reduction and internal fixation, the surgeon must suspect infection or the presence of metal in the joint. Occasionally, avascular necrosis of acetabular fragments causes early collapse and chondrolysis may ensue.
CONCLUSION
The most important decision in the rehabilitation of any fracture is the first one. No amount of therapy can bring back a destroyed joint; therefore, decision making in acetabular trauma is extremely important. The factors determining the prognosis are injury related (the amount of articular damage, the development of avascular necrosis, and the onset of other complications) or surgeon related (adequacy of reduction and iatrogenic complications).
Fractures with hip instability or significant incongruity, especially posterior types, high transverse or T types involving the dome, or fractures with a triangular dome fragment, require accurate open reduction and stable internal fixation allowing early motion. If anatomic reduction is achieved and complications are avoided, good to excellent results can be expected.
The surgery is demanding, has a long learning curve, and is fraught with complications. In addition, the anaesthetic care is difficult and major blood loss is possible. Orthopaedic surgeons should proceed with caution in those cases with which they feel comfortable and refer demanding cases to centres with a pelvic trauma team.
References
Judet R, Judet J, Letournel E. Fractures of the acetabulum: classification and surgical approaches for open reduction. J Bone Joint Surg Am, 1964;46: 1615-46, 1675.
Letournel E. Acetabulum fractures: classification and management. Clin Orthop,
1980;151: 81-106
Letournel E, Judet R. Fractures of
the acetabulum. 2nd ed. Elson RA, translator, editor. New York: Springer; 1993.
Translation of Les fractures du cotyle .
BEAULE, PAUL E. MD, FRCSC; DOREY, FREDERICK J. PHD; MATTA, JOEL M. MD LETOURNEL
CLASSIFICATION FOR ACETABULAR FRACTURES: ASSESSMENT OF INTEROBSERVER AND
INTRAOBSERVER RELIABILITY. Journal of Bone & Joint Surgery - American Volume.
85-A(9):1704-1709, September 2003.