Supracondylar femoral fracture
Supracondylar region area 9cm from knee articular surface.
Bimodal demographic presentation,
- Low energy osteoporotic fractures in elderly patients
- High energy in young patients.
Prior to the early 1970s, most fractures of the distal femur were treated non - operatively. Although there remain indications for nonoperative management of distal femur fractures, most authors suggest surgical intervention.
Radiographs
AP, LAT
May visualize intra articular better with 45 degree obliques. Traction views may help
 |
Common deformities
|
CT scan may be useful in cominuted articular fractures
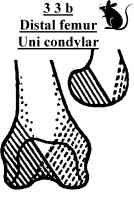
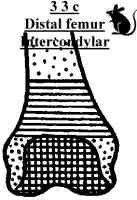
Classification
Most useful AO (AO/ASIF)
 |
AO classification3 = femur 3= Distal metaphysis A - Extraarticular |

(Mouseover above to run animations)
Treatment
Surgical technique and implants have improved considerably leaving very few indications for non operative management of supracondylar fractures.
Non operative
Generally need to look for reason not to operate. Patient unfit for surgery bearing in mind patient may not be fit for prolonged bed rest. Poor bone quality or gross comminution, preventing adequate hold / fixation. In this case best not embarking on operative fixation.
Undisplaced and impacted fractures can be treated non operatively.
- Stable undisplaced impacted fractures - protected weight bearing in hinged cast brace
- Unstable not amenable to fixation - skeletal traction 6-12 weeks followed by hinged knee brace
Complications of non-operative treatment included angular deformity, joint incongruity, knee stiffness, and delayed patient mobility.
Operative treatment
Aims
- reconstruct articular surface
- attach to proximal fragment maintaining mechanical alignment of lower limb
Surgical options/ implants screws ,
- Lag screws - to reconstruct intercondylar split
- 95 degree fixed angle blade plates - technically demanding, rigid fixation (good for good quality bone)
- Dynamic condylar screw (DCS) - Less technically demanding than blade plate
- Condylar Buttress plates - device of choice for comminuted intra-articular fractures, biomechanically weaker than DCS/ blade plate
- Liss plate (less invasive skeletal stabilisation)
- Intramedullary nailing - Supracondylar, retrograde femoral, antegrade femoral, can be used with lag screws for intercondylar fractures
- External fixation - bridging acutely, Fine wire/ ilizarov (rarely long term)
Implant choice depends on
- 1. Fracture (fracture pattern, level, comminution)
- 2. Patient / bone (viz older, poor bone stock and poor hold of rigid implants)
- 3. Surgeon (Implant knowledge/ availability)
Surgical technique
Helfet, David L. MD, Lorich, Dean G. MD, Retrograde Intramedullary Nailing of Supracondylar Femoral Fractures. Clinical Orthopaedics & Related Research. (350):80-84, May 1998.
Placide, Ricky J. MD. Lonner, Jess H. MD. Fractures of the distal femur. Current Opinion in Orthopedics. 10(1):2-9, February 1999.